

One way to achieve cost savings in the CSSD department is to reduce wasted cycle of costs, not just in terms of human labour, but also material costs including packing material, indicators, utilities such as water, electricity, etc. These costs could amount to anywhere between Rs. 300/- to Rs. 500 per set depending on the location and size of the hospital.
Wasted cycles are the result of sets expiring before use or sets being opened only to use few instruments or simply to look for some instruments.
To study this issue, we looked at expired set data at one of our Client Hospital. This 100-bed hospital uses Pivot Smartflow to run their CSSD Department.
Here is what we found:
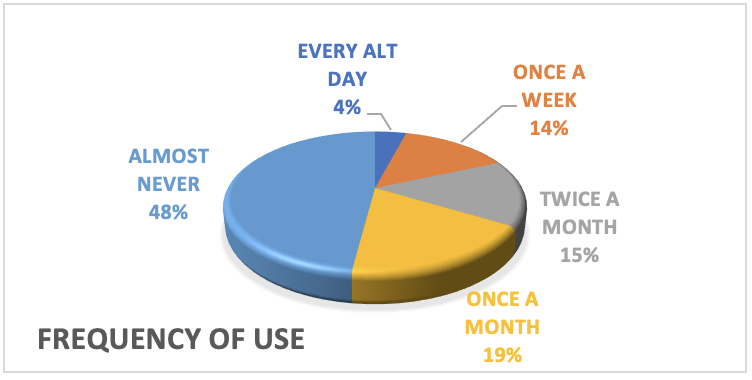
- Only 33% of the sets are used every week or fortnight while a whopping 67% of sets are used only once a month or lesser
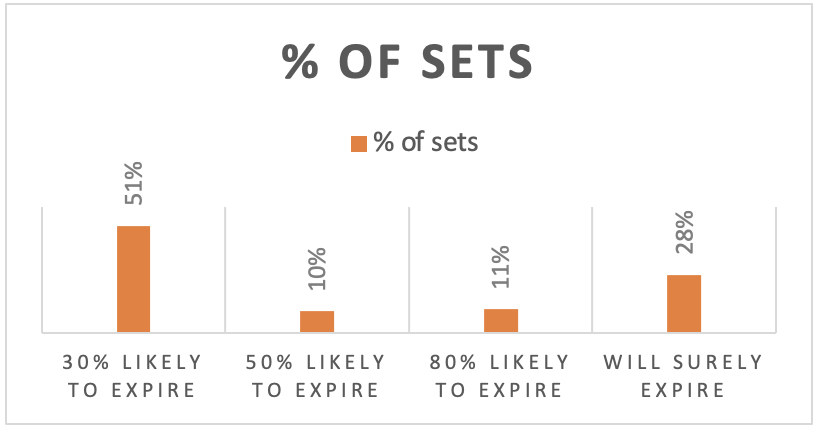
- Almost half the sets have have a higher chance of expiring than being used!
- The hospital had 133 wasted cycles in a quarter or 532 wasted cycles a year just due to Expired Sets translating to Rs. 2 Lakhs of wasted processing per annum.
- For a 300 bedded hospital, this could translate to Rs. 6-8 lakhs per annum on expired sets alone!
- Anecdotal evidence suggests that 1 in 4 sets opened in the Operation Theatre is only partially used (opened for a few instruments alone). If we add wasted costs on account of these sets, the potential wasted reprocessing could amount to over Rs.10 lakhs per annum.
Then there are other considerations:
- Unnecessary wear and tear of instruments due to repeat washing and sterilisation
- Manpower overheads in managing unnecessary volume – not just in CSSD but also in the highly critical operation theatres
How can this data be used to improve?
- Can the hospital evaluate Just-In-Time inventory methods for sets highly likely to expire (i.e. sterilize only when a case is scheduled)?
- Can the hospital share infrequently used sets across their other branch hospitals in the same city, rather than building inventory at each centre?
- Can the hospital look at a pay-per-use model for sets that are infrequently used rather than purchasing these?
I am sure each of these can be evaluated and wasted costs optimized over time.
But moral of the story: Where this is Data, there can be Insights. Where there are Insights, there can be Action. And where there is Action, there can be Savings. One more reason to implement Pivot Smartflow at your hospital Today!
Trackbacks/Pingbacks